
Midlife is a hormone rollercoaster. For many women, the years leading up to the final menstrual period—called perimenopause (a multi‑year transition when estrogen and progesterone fluctuate wildly)—reshape sleep, mood, focus, and how you feel in your own skin. The good news: these changes follow a pattern we can explain and, in most cases, manage effectively without hype.
Perimenopause is a brain–ovary conversation that changes
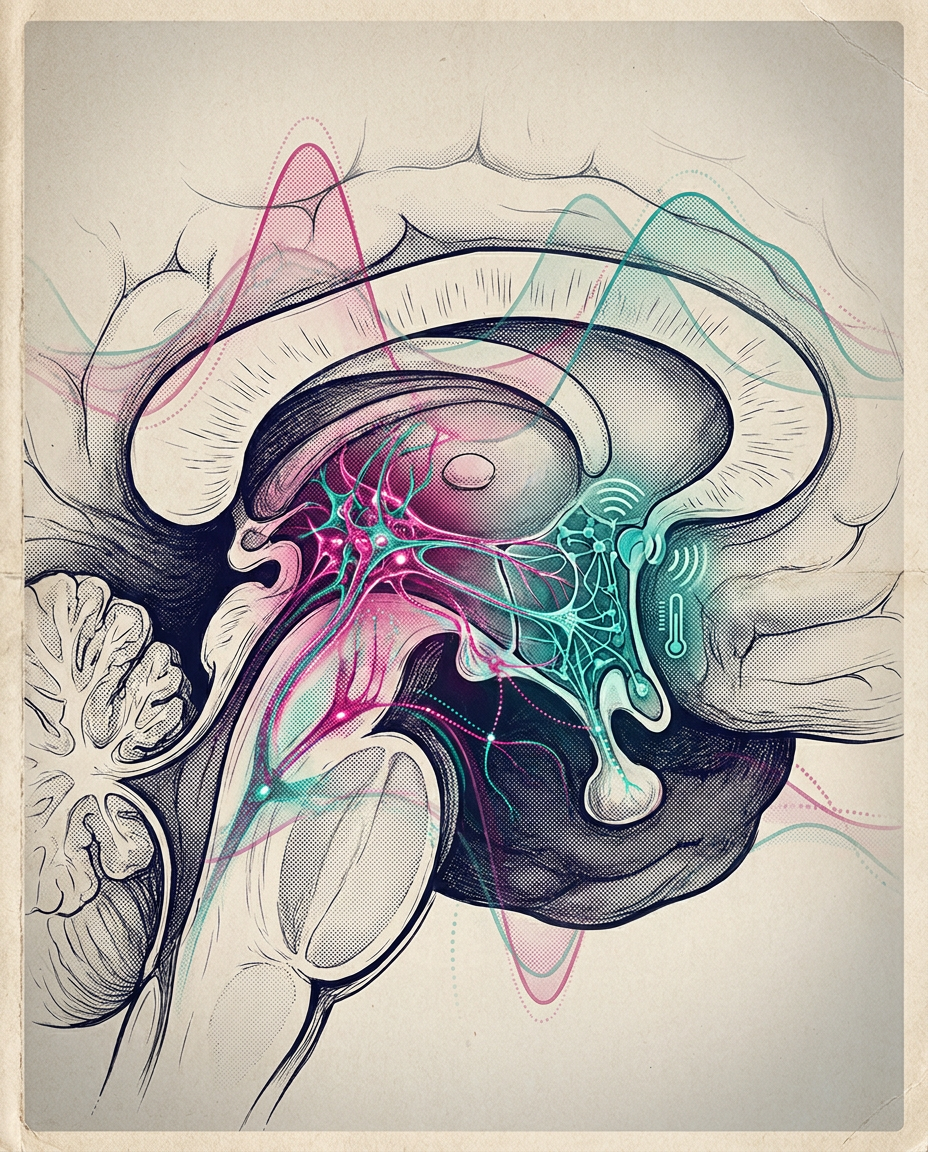
Perimenopause begins when ovarian follicles (the hormone‑producing units in the ovary) start running low. Estradiol (the main estrogen) becomes erratic—surging high, then dropping fast—while progesterone (the hormone that stabilizes sleep and temperature after ovulation) trends lower. These swings confuse the brain’s thermostat. The hypothalamus (your heat‑control center) becomes oversensitive, so small temperature shifts trigger a full‑body flush and sweat. Those hot flashes and night sweats—called vasomotor symptoms, or VMS (sudden episodes of heat with sweating and palpitations)—are the hallmark of the transition.
A specific set of neurons called KNDy neurons (kisspeptin, neurokinin B, and dynorphin—three signaling chemicals that coordinate reproductive rhythms) sit in that thermostat network. When estrogen fluctuates, these neurons fire irregularly and push heat‑dissipation signals. This is more than theory: a 2023 NEJM randomized trial of the neurokinin‑3 receptor blocker fezolinetant—Fraser et al., NEJM, 2023—reduced hot flashes meaningfully versus placebo, which tells us the KNDy pathway is a real driver of symptoms (emerging evidence) [Fraser et al., N Engl J Med, 2023, DOI:10.1056/NEJMoa2213555].
How long does this last? In the large SWAN cohort (a long‑running U.S. study of midlife women), frequent hot flashes persisted a median of 7.4 years, and in some women over a decade, which is why planning matters (well‑established) [Avis et al., JAMA Intern Med, 2015, DOI:10.1001/jamainternmed.2014.8063].
Symptoms touch sleep, mood, cognition, and work
Night sweats fragment sleep. When estradiol drops and progesterone stays low, slow‑wave sleep (deep, restorative sleep) tends to shrink. Many women describe 2–4 awakenings nightly. Chronic sleep loss then feeds anxiety, low mood, and "brain fog"—a cluster of trouble with word‑finding, attention, and working memory. These are real experiences with biological roots, not character flaws.
Risk of new or recurrent depression climbs during the transition. In a prospective cohort, women were about two to three times more likely to develop major depression in perimenopause compared with premenopause (correlation, not proof of causation) [Freeman et al., Arch Gen Psychiatry, 2006, DOI:10.1001/archpsyc.63.4.385]. The mechanism likely blends sleep disruption, stress‑system activation, and sensitivity to hormone swings.
Bone and heart are in the background of all this. Estrogen loss speeds up bone resorption (the breakdown step of bone turnover), which increases fracture risk if nothing is done. In the Women’s Health Initiative—WHI (two large randomized trials of menopausal hormone therapy, or MHT, meaning estrogen with or without a progestogen to protect the uterus)—hip fractures fell with therapy even as other risks rose (well‑established) [Cauley et al., JAMA, 2003, DOI:10.1001/jama.290.13.1729]. Cardiovascular risk also shifts in midlife as LDL‑C (the cholesterol carried by artery‑clogging particles) creeps up and body fat redistributes, which is why fitness, diet quality, and not smoking matter more than ever.
"Hot flashes are biology, not a failure of willpower. When we calm the thermostat, sleep, mood, and focus often follow."
— Dr. Ari Sahebkashaf, THE LONGEVITY LAB MD
What actually works—hormones and nonhormones
For bothersome vasomotor symptoms, MHT—menopausal hormone therapy (physiologic estrogen with a uterine‑protective progestogen if you have a uterus)—is the most effective option (well‑established). Benefits include fewer hot flashes, better sleep, and prevention of bone loss. But benefits come with trade‑offs that depend on age, timing since menopause, and the preparation used.
Randomized trials set the foundation. In the WHI estrogen‑plus‑progestin arm (conjugated equine estrogens 0.625 mg plus medroxyprogesterone acetate 2.5 mg daily), there were modest increases in heart disease, stroke, blood clots, and breast cancer, but fewer hip fractures and less colon cancer during treatment; absolute risks were small per year but meaningful over time (well‑established) [Rossouw et al., JAMA, 2002, DOI:10.1001/jama.288.3.321]. In the estrogen‑alone trial (for women without a uterus), breast cancer did not increase during the trial period, and stroke risk rose modestly (well‑established) [Anderson et al., JAMA, 2004, DOI:10.1001/jama.291.14.1701]. Long‑term follow‑up found no difference in all‑cause mortality with either regimen compared with placebo (well‑established) [Manson et al., JAMA, 2017, DOI:10.1001/jama.2017.11217].
Figure · bar
WHI estrogen+progestin: excess events vs placebo (per 10,000 women-years)
Absolute excess cases while on therapy in the Women’s Health Initiative estrogen+progestin trial [Rossouw et al., JAMA, 2002]. Negative values indicate fewer cases on therapy.
Route and dose matter. Oral estrogen goes through the liver first and raises clotting factors. Transdermal 17β‑estradiol (a skin patch or gel that bypasses the liver) is associated with much lower clot risk than oral preparations in observational studies—suggesting a safer profile for women at elevated clot risk, though this is association, not proven causation (emerging) [Canonico et al., BMJ, 2008, DOI:10.1136/bmj.39555.382134.BE]. The choice of progestogen (the progesterone‑like partner) may also influence breast and clotting risk, but head‑to‑head randomized data are limited (still speculative).
Nonhormonal options help when hormones are not desired or not safe. Neurokinin‑3 receptor antagonists such as fezolinetant cut hot flashes by roughly two episodes per day more than placebo by 12 weeks and improve sleep scores (well‑established for symptom control, long‑term safety still emerging) [Fraser et al., N Engl J Med, 2023, DOI:10.1056/NEJMoa2213555]. Selective serotonin reuptake inhibitors—SSRIs (antidepressants that boost serotonin signaling), and their cousins SNRIs—offer modest reductions in hot flash frequency and severity (emerging evidence from randomized trials and meta‑analyses, effect sizes smaller than MHT). For insomnia, cognitive behavioral therapy for insomnia—CBT‑I (a structured, skills‑based sleep program)—is as effective as sleeping pills over the long term and safer (well‑established in general adult populations) [Espie et al., Lancet, 2012, DOI:10.1016/S0140-6736(12)61464-4]. Many women do best with a combined plan: address the thermostat with hormones or NK3 blockers, protect sleep with CBT‑I habits, and load the skeleton with resistance and impact exercise.
Risk, timing, and personalization drive safer decisions
The "timing hypothesis" says that younger, recently menopausal women may see different cardiovascular effects from estrogen than women decades past menopause. In ELITE (a randomized trial using artery wall thickness—carotid intima–media thickness, or IMT—as a surrogate of atherosclerosis), estradiol started within six years of menopause slowed IMT progression versus placebo; starting 10+ years after menopause did not (emerging; surrogate endpoint, not heart attacks or strokes) [Hodis et al., N Engl J Med, 2016, DOI:10.1056/NEJMoa1505241]. This supports why most guidelines favor starting MHT, if at all, before age 60 or within 10 years of the final period—when benefits are more likely to outweigh risks for healthy women with significant symptoms.
Absolute risk matters more than relative risk. In WHI, the extra events per year were small in absolute terms (for example, ~8 more strokes per 10,000 women‑years with estrogen+progestin) but add up over long use. Your baseline risks—prior blood clots, stroke, heart disease, uncontrolled blood pressure, smoking, or a strong family history of breast cancer—shift the equation. Oral formulations raise clot risk more than transdermal; adding a progestogen is necessary if you have a uterus to prevent endometrial cancer, but progestogens differ and data gaps remain on optimal choice (emerging).
What about cognition and dementia? Evidence is mixed. Starting estrogen years after menopause does not prevent dementia and may increase risk in older starters; starting near menopause has not shown clear cognitive benefit in randomized trials. For now, treat cognitive complaints by fixing sleep, hot flashes, exercise, and alcohol intake rather than chasing estrogen for brain health (emerging, mixed literature).
Duration should be individualized. Many women use MHT for 2–5 years to get through the worst symptoms, then taper. Stopping can be abrupt or gradual; limited evidence suggests tapering may reduce short‑term rebound symptoms, but either approach is acceptable—decide based on preference and how symptoms behave.
- Track symptoms for 2–3 weeks—timing, sleep, triggers. Pattern‑spotting guides the plan.
- Start with foundations: consistent sleep window, morning light, resistance training 2–3 days/week, brisk aerobic work most days, protein at each meal, limit alcohol to at most 1 drink/day, and keep rooms cool at night. These reduce symptom load and protect heart and bone (well‑established for general health).
- If symptoms remain moderate to severe, discuss a trial of transdermal 17β‑estradiol at the lowest effective dose; add micronized progesterone if you have a uterus. Reassess every 6–12 months.
- If hormones are not an option or not preferred, consider fezolinetant or an SSRI/SNRI; combine with CBT‑I for sleep.
- Bone care: get enough dietary calcium (about 1000–1200 mg/day from food and supplements combined, individualized) and vitamin D per lab status; prioritize strength training and impact exercise; consider a DEXA scan (a low‑dose X‑ray that measures bone density) to establish a baseline if you have risk factors.
Disclaimer: This article is intended for educational and informational purposes only and should not be considered medical advice, diagnosis, or treatment. Perimenopause can affect every individual differently, and the most appropriate approach depends on a person’s unique medical history, symptoms, risk factors, lifestyle, and personal preferences. Readers are encouraged to discuss their symptoms and concerns with their own physician or qualified healthcare professional to determine the most suitable and evidence-based approach for their individual situation.
References & Further Reading
- 1. Rossouw JE et al. (2002) Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women's Health Initiative randomized controlled trial. JAMA. https://doi.org/10.1001/jama.288.3.321
- 2. Anderson GL et al. (2004) Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women's Health Initiative randomized controlled trial. JAMA. https://doi.org/10.1001/jama.291.14.1701
- 3. Manson JE et al. (2017) Menopausal hormone therapy and long-term all-cause and cause-specific mortality: the Women’s Health Initiative randomized trials. JAMA. https://doi.org/10.1001/jama.2017.11217
- 4. Fraser GL et al. (2023) Neurokinin 3 receptor antagonism as a treatment for menopausal hot flashes. New England Journal of Medicine. https://doi.org/10.1056/NEJMoa2213555
- 5. Avis NE et al. (2015) Hot flashes and night sweats in midlife women: SWAN study of symptom prevalence and duration. JAMA Internal Medicine. https://doi.org/10.1001/jamainternmed.2014.8063
- 6. Cauley JA et al. (2003) Effects of estrogen plus progestin on risk of fracture and bone mineral density: the Women’s Health Initiative randomized trial. JAMA. https://doi.org/10.1001/jama.290.13.1729
- 7. Canonico M et al. (2008) Postmenopausal hormone therapy and risk of venous thromboembolism: results from the ESTHER study and a meta-analysis. BMJ. https://doi.org/10.1136/bmj.39555.382134.BE
- 8. Hodis HN et al. (2016) Vascular Effects of Early versus Late Postmenopausal Treatment with Estradiol. New England Journal of Medicine. https://doi.org/10.1056/NEJMoa1505241
- 9. Espie CA et al. (2012) A randomized, placebo-controlled trial of online cognitive behavioural therapy for chronic insomnia in the general population. The Lancet. https://doi.org/10.1016/S0140-6736(12)61464-4
- 10. Freeman EW et al. (2006) Associations of the menopausal transition with depressive symptoms: a prospective study. Archives of General Psychiatry. https://doi.org/10.1001/archpsyc.63.4.385
— End of Article —


